CORP ACCOUNTS WITH SPECIAL INSTRUCTIONS
General Rule:
- For LOA request of laboratories and procedures the member is required to send us a copy of the doctor's request with the exact amount of each procedure before we can issue a LOA.
- All approval requests with amount of Php5,000 and above is required to be encoded in Polaris CBMS.
- All approval requests with amount of Php15,000 and above is required to seek approval first of the Polaris team before we can issue LOA.
- OPD-OR availment are deductible in outpatient limit.
Admission Requirements:
- Admission report or Admission order
- Laboratory results if available
Inpatient Discharge Requirements:
- Medical abstract or Medical certificate with the attending physician's signature
- Summary of Account (SOA)
- Itemized charges
- Laboratory results
- OR-tech (if applicable)
- PF should be indicated in the SOA
- Discharge Schedule: Monday to Friday up to 6pm only; Saturday up to 2pm only; Sunday no discharge allowed
Click here to download the computation sheet of Polaris.
For Discharge Approval:
Please send only one email at a time, ensuring it contains all the necessary details and attachments.
Ensure that all attachments are labeled clearly.
The following documents are required for approval:
- Medical Certificate/Abstract/Discharge Note (must include the final diagnosis and the doctor’s signature. For the Discharge Order, the disposition of the patient upon discharge must be included)
- Statement of Account (SOA)
- Approval Template
- Additional documents as requested (e.g., Patient data, laboratory results, etc. As per the approver’s instructions, Medical Officers may send the Medical Certificate/Abstract, SOA, and Approval Template initially for computation.)
Send the approval to the following email addresses:
- coo@polaris-finance.com; support@polaris-finance.com; info@polaris-finance.com; insurance@polaris-finance.com; operation@polaris-finance.com; xguirao@polaris-finance.com; helpline@polaris-finance.com
For OPD-OR Approval:
Approval is required for amounts of 15,000 and above.
Please send only one email at a time with complete details and an attachment.
Ensure that the attachment is labeled appropriately.
The following document is required for approval:
- Doctor’s request (must include the final diagnosis and the doctor’s signature)
Send the approval to the following email addresses:
- coo@polaris-finance.com
- support@polaris-finance.com
- info@polaris-finance.com
- insurance@polaris-finance.com
- operation@polaris-finance.com
- xguirao@polaris-finance.com
- helpline@polaris-finance.com
- tpa@polaris-finance.com
- gm@polaris-finance.com
CHRONIC DERMATOSES - COVERED (POLARIS FINANCIAL-PIONEER MARINE HELLAS S.A)
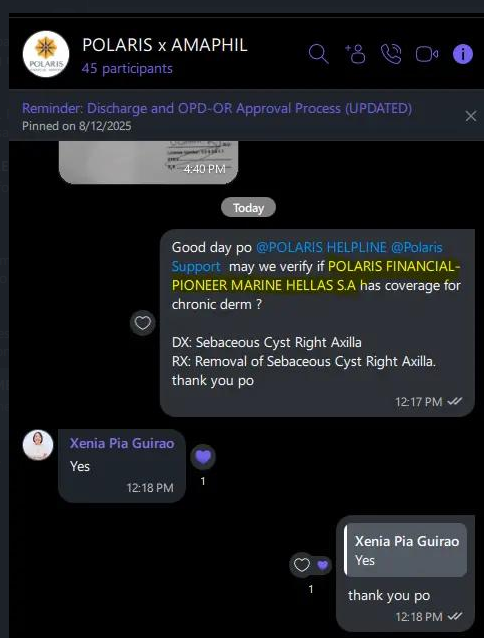
DETAILS TO ASK TO THE PROVIDER DURING LOA REQUEST
Please provide the following details:
1. Last consultation (date)
2. Name of doctor on last consult
3. Medications
4. Itemized price of lab tests
5. Copy of doctor's request
RULES AND GUIDELINES IN LOA APPROVAL
1. Request for coverage must come from accredited physician with valid loa for consult (members cannot request for procedures on their own)
Do not approve requests for lab/diagnostic procedures without this or from non-accredited doctors
2. No approval for non-accredited but accepting physicians
3. No requests for approval for loa ordered for laboratory/diagnostic procedures withour prior consultation with the accredited physician
4. If md is accredited but the patient did not pass thru our process (ie loa facilitated consult) and paid the pf, then did not pass thru our system and there should be no approval for the request for lab or diagnostic
5. No approval for previous requests for lab/dianostic procedures from md when the patient was still with another hmo (requested when the member was still with former hmo)
6. Re-assess request that were ordered more than 2 months ago (request must be current)
ADDITIONAL REQUIREMENT:
Request a copy of the doctor's request and the exact amount or each procedure.
REQUEST APPROVAL FORMAT
Member's Name:
Age:
Gender:
Company Name:
Facility:
Requesting Doctor's Name:
Doctor's Specialization:
Date of Consultation with the Requesting Doctor:
Prior Consult Chief Complaint:
Diagnosis:
Note: If it is an existing Chronic Disease/PEC, since when that member was diagnosed with this and what were his/her medications:
Requested Tests:
Incurred Utilization:
PEC limit/MBL per illness:
Plan Category:
ROOM AND BOARD UPGRADE PROVISION
Request Certificate of isolation and/or certificate of room non-availability for the application of room waiving.
PROVISION ON INCREMENTAL CHARGES
(Rate of room occupied – room and board plan benefit) x (no. of days confined)
Plus 25% of net hospital bills if upgrading one (1) level: Ward to Semi-Private
Plus 35% of the net hospital bills two (2) levels: Ward to Private
(Not applicable for Suite room upgrade)
HC&D ADMISSION REPORT TEMPLATE
PROVIDED LIST OF PEC:
| Tumor/Cyst of Internal Organs |
| Hemorrhoids/Anal Fistula |
| Diseased tonsils and sinus conditions requiring surgery |
| Cataract/Glaucoma |
| Pathological Abnormalities of nasal septum or turbinates |
| Goiter and other thyroid disorders |
| Hernia/Benign Prostatic Hypertrophy |
| Endometriosis |
| Asthma/Chronic Obstructive Lung disease |
| Epilepsy |
| Spinal column abnormalities |
| Tuberculosis |
| Cholecystitis |
| Gastric or Duodenal ulcer |
| Hallux valgus |
| Hypertension and other Cardiovascular diseases |
| Calculi of the urinary system |
| Tumors/Cyst on skin, muscular tissue, bone or any form of blood dyscracias |
| Diabetes Mellitus |
| Cerebrovascular Accident/Transient Ischemic Attack |
| ENT conditions requiring surgery |
| migraine |
| cirrhosis of the liver / fatty liver |
| cholelithiasis |
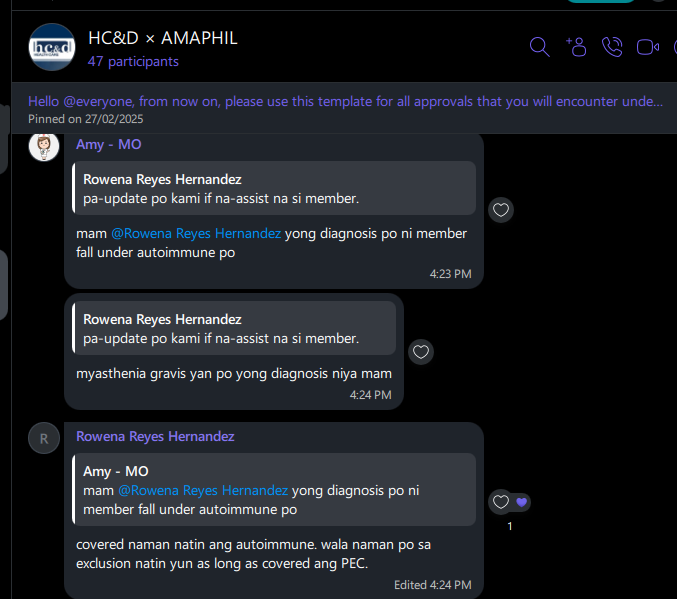
"covered naman natin ang autoimmune. wala naman po sa exclusion natin yun as long as covered ang PEC." - Rowena Hernandez
All availment amounting Php10,000 and above need to have approval from paramount before issuing loa (please email to paramount for documentation).
ROOM AND BOARD UPGRADE PROVISION
Request Certificate of isolation and/or certificate of room non-availability for the application of room waiving.
PROVISION ON INCREMENTAL CHARGES
35% incremental charges
INPATIENT PF COMPUTATION
PF counting is the same with room and board counting (start counting the day after admission).
Computation Sheet needs to be accomplished and send to Paramount team upon request of approval in their end.
Click here to download the computation sheet.
Email Address of the Paramount approvers:
catalina.pamiroyan@paramount.com.ph
naome.lucernas@paramount.com.ph
ACCIDENT AVAILMENT REQUIREMENTS
Upon admission to ER, required to send incident report (IR), POLICE REPORT, OR-CR, DRIVER'S LICENSE
If the patient cannot provide all the requirements, he/she needs to send us a copy of signed waiver.
REMINDERS:
 Incident report is required for all animal bite or scratch cases, regardless of the type of availment.
Incident report is required for all animal bite or scratch cases, regardless of the type of availment.
Incident report is also required for any trauma-related diagnoses, regardless of availment type.
Stabilization fees are not covered (as indicated in the list of non-covered items).
Always request the actual itemized billing for all emergency room (ER) cases.
For Paramount accounts involving MRI or CT scan, coverage is plain only, unless otherwise specified in the Schedule of Benefits (SOB).
Chief complaint of blurred vision is not covered.
Tension headache is not covered.
Physical therapy coverage is limited to basic PT sessions only.
Save a copy of the Paramount approval using the file naming format: TRN_LOA_MEMBER NAME.
 Upload the file here: Google Drive Folder
Upload the file here: Google Drive Folder


CHATS/EMAIL REFERENCE OF CORP VERIFICATIONS
| DATE OF ENDORSEMENT | MODE OF ENDORSEMENT | CORP - FIRST LIFE | DETAILS | REMARK |
| 7-Jun-2024 | VIBER | FIRST LIFE-GTS INSURANCE BROKERS 2023-2024 | GENE XPERT COVERAGE | COVERED AS PER LYVI OPIANO |
| 5-Jun-2024 | VIBER | FIRST LIFE-SCHOOL INN CORP. | PRP COVERAGE | COVERED AS PER LYVI OPIANO |
| 9-Jun-2024 | VIBER | FIRST LIFE- NHA PROVIDENT FUND ASSOCITION INC. | COST OF VACCINE COVERAGE | NOT COVERED AS PER MAESHEIL PADASAS |
| 13-Jun-2024 | VIBER | FIRST LIFE - UNIVERSAL ROBINA CORPORATION MEAT AND CANNING DIVISION NEW EMPLOYEES WORKERS UNION LABO | ANIMAL SCRATCH COVERAGE | COVERED AS PER HAZEL EMBESTRO |
| 19-Jun-2024 | VIBER | FIRST LIFE-PCIEERD | ANIMAL SCRATCH COVERAGE | COVERED UP TO LIMIT AS PER MS. LIEZEL OF FIRST LIFE |
| 15-Jun-2024 | VIBER | FIRST LIFE- NHA PROVIDENT FUND ASSOCITION INC. | EOR NOT COVERED | NOT COVERED AS PER per MS. LYVI OPIANO |
| 1-Jul-2024 | VIBER | FIRST LIFE-GTS INSURANCE BROKERS 2023-2024 | PT COVERAGE | COVERED UP TO MBL AS PER MAESHEIL PADASAS |
| 3-Jul-2024 | VIBER | FIRST LIFE-POINT AD, INC. | Animal bite/scratch | covered up to MBL as per Ms. Lyvi Opiano |
| 27-Jul-2024 | VIBER | FIRST LIFE - NATIONAL MUSEUM | Leptospirosis | COVERED AS PER MS. LYVI |
| 27-Jul-2024 | VIBER | FIRST LIFE - OFFICE OF THE OMBUDSMAN (EMPLOYEE) | AUTOIMMUNE DSES COVERAGE (MYOSITIS) | COVERED AS PER MS. LYVI |
| 9-Sep-2024 | VIBER | FIRST LIFE-PIPOLS SYNERGY MANAGEMENT SERVICES, INC. (MANPOWER) | ANTI RABIES VACCINE for animal bite or scratch not covered | No coverage for anti rabbies vaccine - Lyvi |
| 17-Jul-2024 | VIBER | FIRST LIFE - OFFICE OF THE OMBUDSMAN (EMPLOYEE) | ERROR OF REFRACTION - NOT COVERED | ERROR OF REFRACTION |
| 24-Sep-2024 | VIBER | FIRST LIFE - URC - CANLUBANG PLANT EMPLOYEES UNION (CPEU OLALIA) | SCRATCH - COVERED | SCRATCH - FIRST LIFE - URC - CANLUBANG PLANT EMPLOYEES UNION (CPEU OLALIA).jpg |
| 24-Sep-2024 | VIBER | FIRST LIFE - URC - LABOR UNION | AUTOIMMUNE DSES COVERAGE (RHEUMARHOID A.) - Covered | AUTOIMMUNE DSES COVERAGE (RHEUMARHOID A.) - FIRST LIFE - URC - LABOR UNION.jpg |
| 27-Aug-2024 | VIBER | ALL FIRST LIFE | HEPA B - NOT COVERED | HEPA B - ALL FL ACCOUNTS.PNG |
| 27-Sep-2024 | VIBER | FIRST LIFE - JMD PERSONNEL MANAGEMENT SOLUTIONS CORP. | PEC COVERAGE - COVERED TO ALL PLANS | PEC COVERAGE - FIRST LIFE - JMD PERSONNEL MANAGEMENT SOLUTIONS CORP. .PNG |
| 6-Sep-2024 | VIBER | FIRST LIFE - URC - LABOR UNION | ANIMAL SCRATCH COVERAGE | COVERED PER MAAM HAZEL EMBESTRO; VIBER FL |
| 16-Oct-2024 | VIBER | FIRST LIFE-PRUDENTIALIFE GROUP OF COMPANIES | PT COVERAGE | COVERED UP TO 12 SESSION PER MS. ANNE POLICARPIO |
| 15-Oct-2024 | VIBER | FIRST LIFE - MANILA METRO RAIL TRANSIT | AUTOIMMUNE DISEASES | COVERED PER MS. LYVI |
| 23-Oct-2024 | VIBER | FIRST LIFE - OFFICE OF THE OMBUDSMAN (EMPLOYEE) | animal scratch covered -sir Jopeth via FL viber GC | |
| 6-Nov-2024 | VIBER | FIRST LIFE - EXECUTIVE GENESIS SERVICES | covered animal scratch | verification from mam Lyvi |
| VIBER | FIRST LIFE - OFFICE OF THE OMBUDSMAN | AUTOIMMUNE DISEASES ; PET SCAN | COVERED | |
| VIBER | FIRST LIFE - OFFICE OF THE OMBUDSMAN (EMPLOYEE) | ANIMAL SCRATCH COVERED -sir Jopeth via FL viber GC | ||
| 26-Nov-2024 | VIBER | FIRST LIFE-GRAINPRO PHILIPPINES, INC. | Animal scratch covered as per mam hazel | |
| 29-Nov-2024 | VIBER | FIRST LIFE-PCIEERD | Autoimmune diseases covered under FIRST LIFE-PCIEERD as per mam lyvi | |
| 29-Nov-2024 | VIBER | FIRST LIFE-DOWELL CONTAINER AND PACKAGING CORP. 2023-2024, | Sputum Gene Expert covered | |
| 5-Dec-2024 | VIBER | FIRST LIFE - DON BOSCO MANDALUYONG ALUMNI ASSOCIATION | w/ coverage for animal scratches up to 40k | |
| 11/26/2024 | VIBER | ALL FIRST LIFE | ANIMAL SCRATCH | ANIMAL SCRATCH IS COVERED AS LONG AS WITH ANTI RABIES COVERAGE |
FIRST LIFE- PPA PANTALAN NCR SOUTH
FIRST LIFE - CSSDO EMPLOYEES MULTI PURPOSE COOPERATIVE / FIRST LIFE - FLH EMPLOYMENT SERVICES
FIRST LIFE - SUBURBIA AUTOMOTIVE VENTURES INC. (MANAGE CARE)
FIRST LIFE - SUBURBIA AUTOMOTIVE VENTURES INC. (MANAGE CARE) ANIMAL BITE For reimbursement po. As per Ms. Aiza Pili
ALL ACCOUNTS
1. Procedure with inner limit in SOB follow the SOB
REVISED 09/10/2024: If in the event that the required procedure is not in the SOB, we will deny approval. However, if the Insured member will provide proof that the procedure is part of the take-over provision then we will accommodate and if the procedure will fall under the new modality, the approved limit is Php5,000.
2.TB case - covered tuberculin test only
3. Animal scratch/bite category II and up - covered
INCREMENTAL CHARGES IN CASE OF ROOM UPGRADE
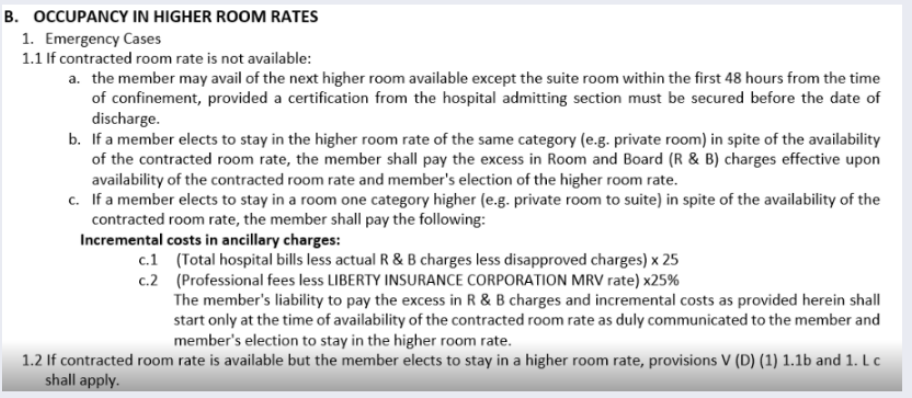
LIBERTY.INSURANCE-LANDBANK EMPLOYEES ASSOCIATION - AUTOIMMUNE 50% OF ABLDATE VERIFIED MODE OF ENDORSEMENT CORP - LIBERTY DETAILS REMARKS 4-Jun-2024 VIBER LIBERTY INSURANCE-Welfarefund Employees Association ANIMAL SCRATCH COVERAGE COVERED AS PER LEILANI MARQUEZ 23-May-2024 VIBER LIBERTY - Manila International Freight Forwarders, Inc. (MIFFI) ANIMAL SCRATCH COVERAGE COVERED AS PER LEILANI MARQUEZ 26-Apr-2024 EMAIL LIBERTY.INSURANCE.GENSAN-LOCAL GOVERNMENT UNIT GENERAL SANTOS CITY AUTOIMMUNE DSES COVERAGE COVERED AS PER TONI MATIC 5-Jun-2024 EMAIL LIBERTY INSURANCE-WERDENBERG INTERNATIONAL CORPORATION SLEEP DISORDER NOT COVERED AS PER TONIE MATIC 7-Jun-2024 VIBER LIBERTY INSURANCE-Liwayway Marketing Corporation UPON ADMISSION TO DISCLOSE MBL OF PT AS PER MA'AM IZA 7-Jun-2024 VIBER LIBERTY INSURANCE-WERDENBERG INTERNATIONAL CORPORATION ANIMAL BITE COVERAGE NO COVERAGE AS PER MS. TONIE MATIC 11-Jun-2024 VIBER LIBERTY - THICK AND THIN AGRI-PRODUCTS, INC. ANMAL SCRATCH COVERAGE COVERED AS PER LEILANI MARQUEZ 14-Jun-2024 VIBER LIBERTY GSIS-KAPISANAN NG MGA MANGGAGAWASA SA GSIS AUTOIMMUNE DSES COVERAGE COVERED AS PER MS NANCY DELA CRUZ 24-Jun-2024 VIBER LIBERTY GSIS-KAPISANAN NG MGA MANGGAGAWASA SA GSIS SLEEP STUDY COVERED COVERED AS PER MS NANCY DELA CRUZ 25-Jun-2024 VIBER LIBERTY - Philippine Council for Agriculture and Fisheries Employees Association NO COVERAGE FOR GENE XPERT We will cover tubercullin test for any TB related test. - AS PER MAM NANCY 24-Jun-2024 VIBER LIBERTY INSURANCE-Welfarefund Employees Association COVERAGE FOR ANIMAL BITE S/B WITHIN 24HRS AS PER MS LEI 2-Jul-2024 VIBER LIBERTY.INSURANCE-GSIS-KAPISANAN NG MGA MANGGAGAWASA SA GSIS PET SCAN COVERAGE COVERED UP TO MBL AS PER MS NANCY 1-Jul-2024 VIBER LIBERTY.INSURANCE.GENSAN-LOCAL GOVERNMENT UNIT GENERAL SANTOS CITY SLEEP STUDY COVERAGE COVERED UP TO MBL AS PER MS TONIE 28-Jun-2024 VIBER LIBERTY INSURANCE-ASIAN TRANSMISSION CORPORATION COVID ANTIGEN covid antigen ok to proceed as long as may signs and symptoms yung pt AS PER MS LEI MARQUEZ 8-Jul-2024 VIBER LIBERTY GSIS-KAPISANAN NG MGA MANGGAGAWASA SA GSIS EPILEPSY AS PER INSTRUCTION BY CLYDE 8-Jul-2024 VIBER LIBERTY GSIS-KAPISANAN NG MGA MANGGAGAWASA SA GSIS GSIS * LIWAYWAY / Autoimmune, Scratch, Genetic/Hereditary covered AS PER INSTRUCTION BY CLYDE 8-Jun-2024 VIBER LIBERTY INSURANCE-Maynilad Water and Sewerage Union-PTGWO SCRATCH CATEGORY 3 COVERED AS PER MS LEI MARQUEZ 8-Jul-2024 VIBER LIBERTY INSURANCE-Liwayway Marketing Corporation GSIS * LIWAYWAY / Autoimmune, Scratch, Genetic/Hereditary AS PER INSTRUCTION BY CLYDE 27-Jul-2024 VIBER LIBERTY INSURANCE - OFFICE OF THE SOLICITOR GENERAL Leptospirosis COVERED AS PER MS. NANCY 1-Aug-2024 VIBER LIBERTY INSURANCE-Maynilad Water and Sewerage Union-PTGWO SCRATCH CATEGORY 2 COVERED AS PER MS. NANCY 17-Aug-2024 VIBER LIBERTY INSURANCE-BIOCARE LIFESCIENCES INC. AUTOIMMUNE DSES COVERAGE COVERED AS MS. TONIE 19-Aug-2024 VIBER LIBERTY INSURANCE-SAN PEDRO LAGUNA LGU PERIPHERAL INJECTION THERAPY NOT COVERED AS PER MS. NANCY - OPD medicine is not covered. Only physical Thepathy. 19-Aug-2024 VIBER LIBERTY INSURANCE-SAN PEDRO LAGUNA LGU ACCUPUNTURE Therapy NOT COVERED AS PER MS. TONIE 22-Aug-2024 VIBER LIBERTY INSURANCE-ALTITUDE MARITIME TRAINING AND ASSESSMENT CENTER INC. ANIMAL BITE/SCRATCH COVERED AS PER MS. TONIE CATEGORY 2 AND UP 27-Aug-2024 VIBER LIBERTY INSURANCE-Maynilad Water and Sewerage Union-PTGWO PT COVERAGE COVERED UP TO MBL IF NO INDICATED LIMIT AS PER MS. LEI CONTACTED BY SIR GERICK 9-Sep-2024 VIBER LIBERTY INSURANCE-RTU-KAWANI MULTI-PURPOSE COOPERATIVE ANIMAL SCRATCH COVERAGE CATEGORY 2 ABOVE COVERED - LEI MARQUEZ 10-Sep-2024 VIBER LIBERTY INSURANCE-Liwayway Marketing Corporation SLEEP STUDY COVERED AS PER MS. NANCY - CHECK EMAIL ENDORSEMENT 17-Oct-2024 VIBER LIBERTY INSURANCE - JORGEN ADVERTISING INC., AUTOIMMUNE DISEASES NO COVERAGE FOR AUTOIMMUNE DSE PER MS. LEI MARQUEZ 10/25/2024 VIBER LIBERTY INSURANCE - COMELEC EMPLOYEES DEVELOPMENT COOPERATIVE-CEDC ADMISSION: COVID For COVID cover, it should be RT-PCR positive result and not Antigen test. -maam nancy from Liberty Gc 29-Oct-2024 VIBER LIBERTY - INDUSTRIAL TECHNOLOGY DEVELOPMENT INSTITUTE RAPID ANTIGEN TEST Not covered , RT-PCR only if with symptoms -as per sir gerick verified to Ms. Lei Marquez 1-Nov-2024 viber LIBERTY INSURANCE-ONEIMUS JOB CONTRACTING SERVICES ANIMAL BITE COVERAGE Covered 20k only per Ms. Lei Marquez 2-Nov-2024 VIBER LIBERTY INSURANCE-Welfarefund Employees Association Passive and active vaccines for treatment of tetanus, animal bites, snake bites mam Lei Marquez: let's initially cap the limit up to 30k, will review the documents and revert on this 31-Oct-2024 VIBER LIBERTY INSURANCE-ONEIMUS JOB CONTRACTING SERVICES first dose coverage - Anti rabies up to 20k only per maam Lei of Liberty viber GC VIBER LIBERTY INSURANCE-ALTITUDE MARITIME TRAINING AND ASSESSMENT CENTER INC. PEC OVERED per maam Lei of Liberty viber GC 16-Nov-2024 VIBER LIBERTY INSURANCE-ISLAND RESORT TOUR SERVICES INC animal scratch category 3 covered 16-Nov-2024 VIBER LIBERTY - COUNTRYSIDE BUILDERS MULTI-PURPOSE COOPERATIVE (CBMPC) Pt session is up to 12 per mam Lei Liberty viber GC 22-Nov-2024 VIBER LIBERTY INSURANCE - GUADALUPE COMMUNITY MULTI-PURPOSE COOPERATIVE Endoscopic procedures, IP & OP- 5k only, confirmed to liberty. 22-Nov-2024 VIBER LIBERTY INSURANCE - SAMAHAN PARA SA IKAUUNLAD NG MGA KAWANI NG AGHAM AT TEKNOLOHIYA (SIKAT) AUTO-IMMUNE NOT COVERED 25-Nov-2024 VIBER LIBERTY INSURANCE - NAFC- DA MULTI PURPOSE COOPERATIVE covered animal scratch category 2 and up 27-Nov-2024 VIBER LIBERTY INSURANCE - INLAND AQUATIC RESEARCH AND DEVELOPMENT (IARRD) IF ER CASE AND CATEGORY 2 UP PER SIR GERICK_MAM LEI OF LIBERTY 29-Nov-2024 VIBER LIBERTY INSURANCE - OPTIONS - PRIMERA MULTI-PURPOSE COOPERATIVE For primera this is the same as the other agencies like cavcon golden manna and oneimus meron coverage up to specified limit. Extended to cover scratches if CAT 2 and above. Kindly accommodate our member as advised by sir jerome PER MAM LEI OF LIBERTY VIBER GC / UP TO 20K 5-Jul-2024 VIBER LIBERTY.INSURANCE-GSIS-KAPISANAN NG MGA MANGGAGAWASA SA GSIS COVID 19 INFECTION for RT PCR If screening not covered. If positive we can reimburse. 
| DATE | MODE OF ENDORSEMENT | CORP - HC&D | DETAILS | REMARKS |
| 9/11/2024 | VIBER | ALL HC&D ACCOUNTS | ANIMAL SCRATCH | covered, we do consider scratch under animal bite - Rowena |
| 11/12/2024 | VIBER | HC&D - DEPT. OF SCIENCE AND TECHNOLOGY - SCIENCE EDUCATION INSTITUTE | RADIATION THERAPY | Covered up to 12 Session under therapeutic procedures radioactive-Rowena |
| 12/9/2024 | VIBER | HC&D - F.F. INTERNATIONAL MANUFACTURING CORPORATION | RADIOTHERAPY | Covered up to 12 Session under therapeutic procedures radioactive-Rowena |
| DATE OF ENDORSEMENT | MODE OF ENDORSEMENT | CORP - STARDUST | DETAILS | REMARKS |
| 4-Jul-2024 | VIBER | Stardust-Infant Wears Inc. | PHYSICAL THERAPY COVERAGE | Effective immediately, absolutely no PT covered AS PER S PIA BRIEN |
| DATE OF ENDORSEMENT | MODE OF ENDORSEMENT | CORP - LAWINA/RIBAI | DETAILS | REMARKS |
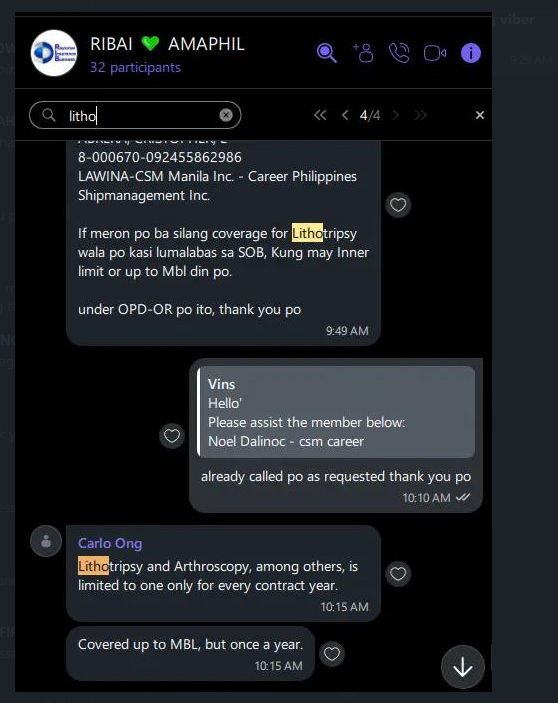
| 13-Jul-2024 | VIBER | LAWINA-CSM Manila Inc. - Career Philippines Shipmanagement Inc. | TETANUS VACCINE | COVERED AS PER SIR CARLO |
| 13-Jul-2024 | VIBER | LAWINA-CSM MANILA, INC. - SENATOR CREWING (MANILA), INC | TETANUS VACCINE | COVERED AS PER SIR CARLO |
| 8-May-2024 | VIBER | LAWINA-HARREN & PARTNER CREW MEDICAL INSURANCE | Animal bite | First dose only |
| 27-May-2024 | VIBER | RIB-CASA BELLA HOME AND LIVING CORP | ESWL | ESWL - covered up to MBL |
| N/A | N/A | *Intermodal Shipping Inc | ER CASE | K-line group Emergency case - IP LIMIT - for UK account charge to OP limit |
| N/A | N/A | *New Filipino Maritime Agencies Inc | ||
| N/A | N/A | *Ventis Maritime Corp - KRBS | ||
| N/A | N/A | *Veritas Maritime Corporation | ||
| N/A | N/A | *Ventis Maritime Corp - SGP | ||
| N/A | N/A | *K LNG Maritime Services Inc - KMSM | ||
| N/A | N/A | *Ventis Maritime Corp - SPT | ||
| N/A | N/A | *Ventis Maritime Corp - KMSM | ||
| N/A | N/A | *K LNG Maritime Services Inc - UK | ||
| 2-Nov-2024 | VIBER | LAWINA-PGA Upstart-Gorilla Geo Industries, Inc | for TB Genexpert procedure - DX pulmonary tuberculosis | It’s covered in their pre-existing. Thanks. per Sir Carlo ong via RIBAI gc |
| 2-Aug-2024 | VIBER | LAWINA-CSM MANILA, INC. - SENATOR CREWING (MANILA), INC | First dosed of anti rabies up to 10k | |
| 19-Jun-2024 | VIBER | LAWINA-CSM Manila Inc. - Career Philippines Shipmanagement Inc. | 10k Limit for Animal Bite |
Email Subject: Additional Exclusion & Revision of Benefits
| from: | Mark Paquita <mark.paquita@rayomarinsurance.com> |
Hi Ma’am / Sir,
Kindly see the below changes in benefits and additional exclusion for the following accounts as stated below:
- Sexually transmitted diseases such as AIDS, Hepatitis B, Condyloma, Gonorrhea, Syphilis, Herpes, etc., and their attendant complications.
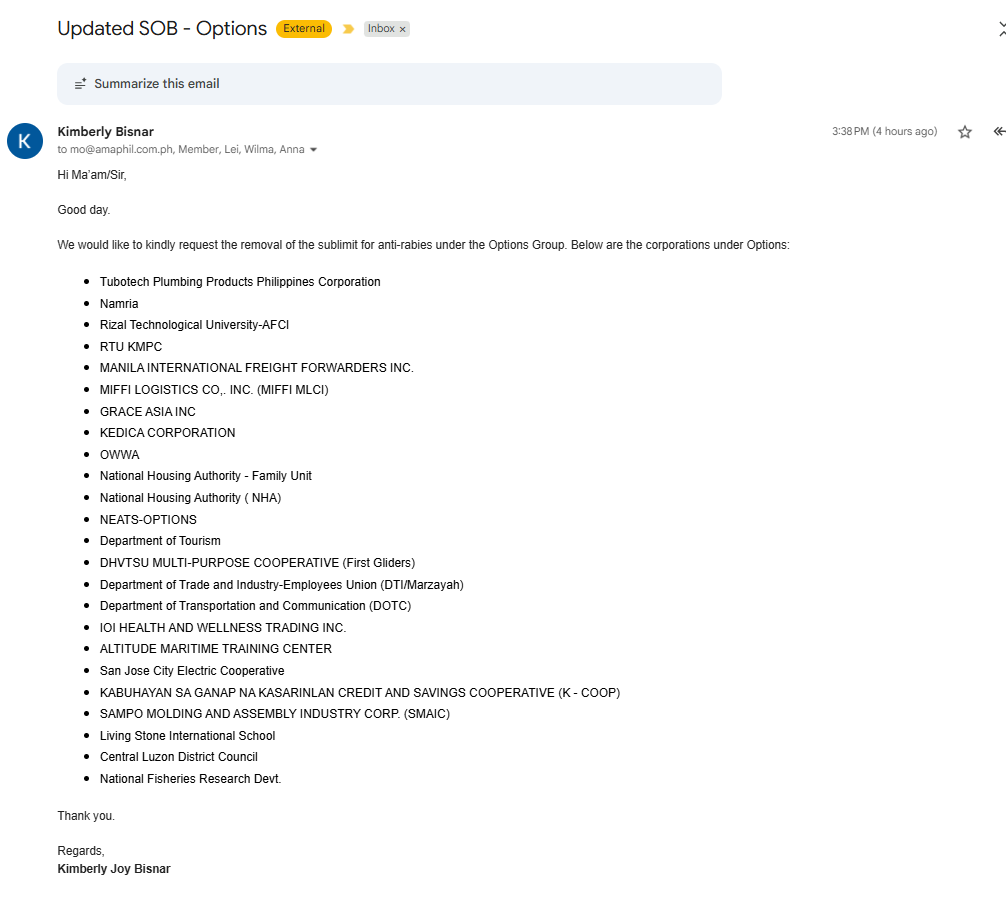
The additional exclusion above applies to the following corporations:
- BIODIVERSITY MANAGEMENT BUREAU
- OPTIONS-DICT
- OPTIONS-DNEA
- GENERAL MARIANO TECHNOLOGICAL HIGH SCHOOL ( GMATHS )
- GRACE ASIA INC
- KEDICA
- MANILA INTERNATIONAL FREIGHT FORWARDERS INC.
- MIFFI LOGISTICS CO,. INC.
- NAMRIA
- OPTIONS NEATS
- NATIONAL HOUSING AUTHORITY
- NATIONAL HOUSING AUTHORITY FAMILY UNIT
- OWWA
- PEA-OPTIONS
- RTU-KMPC
- RTU-AFCI
- Tubotech Plumbing Products Philippines Corporation
- DHVTSU MULTI-PURPOSE COOPERATIVE
- Department of Tourism
- Department of Trade and Industry-Employees Union
- Department of Transportation and Communication
- IOI HEALTH AND WELLNESS TRADING INC.
- ALTITUDE MARITIME TRAINING CENTER
- San Jose Electric Cooperative
- KABUHAYAN SA GANAP NA KASARINLAN CREDIT AND SAVINGS COOPERATIVE (K - COOP)
- LIVING STONE INTERNATIONAL SCHOOL
- Central Luzon District Council of the Assemblies of God
PEME Amounts for Kline Group
| Account Code | Corporates | Member Type | Peme Amount |
| 294 | One Sea Solutions | Principal | 5,000 |
| 669 | K LNG Maritime Services Inc-KMSM | Principal | 5,000 |
| 686 | Ventis Maritime Corp-KMSM | Principal | 5,000 |
| 284 | Ventis Maritime Corp - KRBS | Principal | 10,000 |
| 283 | Newfil Maritime Agencies Inc | Principal | 10,000 |
| 324 | Veritas Maritime Corporation | Principal | 10,000 |
| 282 | Intermodal Shipping Inc | Principal | 10,000 |
LAWINA-CSM Manila Inc. - Career Philippines Shipmanagement Inc.
EWSL - COVERAGE
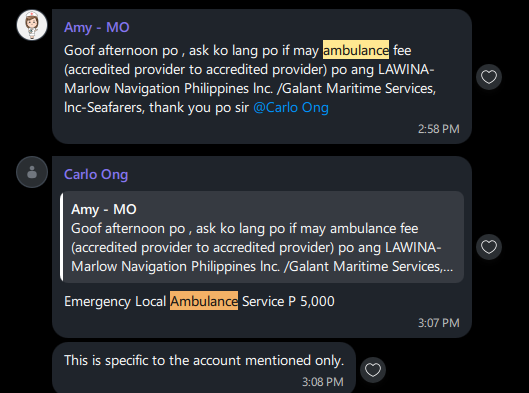
LAWINA-Marlow Navigation Philippines lnc. /Galant Maritime Services, lnc-Seafarers
Emergency Local Ambulance Service P 5,000
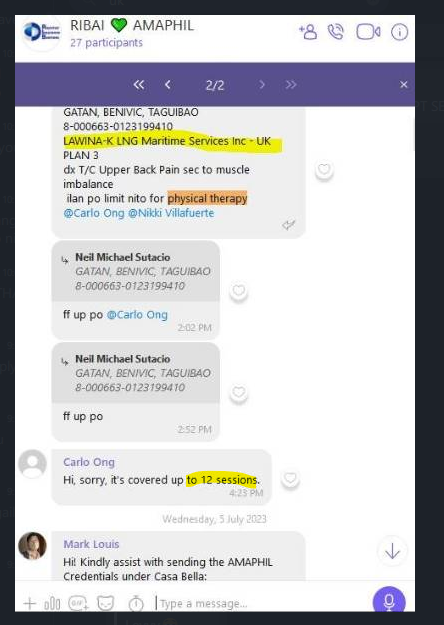
LAWINA-K LNG Maritime Services Inc - UK
12PT SESSION
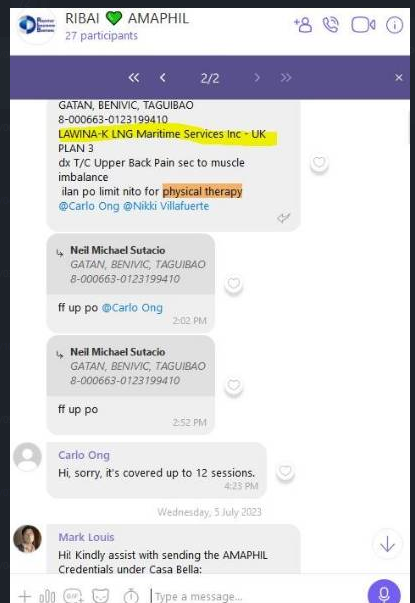
LAWINA-K LNG Maritime Services Inc - UK
Physical Therapy coverage up to 12 sessions
LAWINA-New Filipino Maritime Agencies, Inc.
Physical Therapy coverage
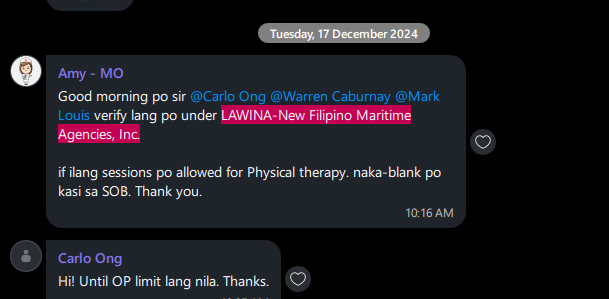
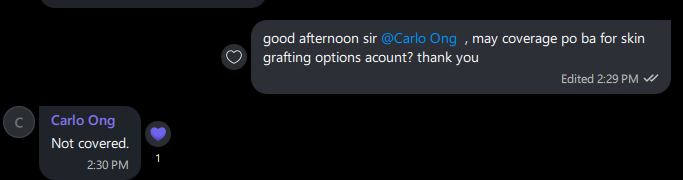
LAWINA - OPTIONS
SKIN GRAFTING NOT COVERED
LAWINA - OPTIONS
covid coverage

anti-rabies vaccine and its administration - up to MBL
| DATE OF ENDORSEMENT | MODE OF ENDORSEMENT | CORP - FIRST LIFE | DETAILS | JUSTIFICATION |
| Sep 26, 2024 | VIBER | BUSINESS MACHINES CORPORATION | PT COVERAGE - BASIC PT ONLY UP TO 12 SESSIONS | PT COVERAGE - BUSINESS MACHINES CORPORATION.PNG |
Special Approval Meizel Barquilla
Requesting approval for Meizel Barquilla for access to Medical City Makati Waltermart Branch
WITH ACCESS TO ALL MAJOR HOSPITAL/CLINICS
| EXCLUSIONS FOR HOSPITALIZATION BENEFIT |
| No benefit shall be made for any loss resulting from or cause by: |
| 1. Self-inflected injuries; nervous or mental disease or disorder; pregnancy, childbirth, miscarriage, abortion or any complications of any of these; congenital deformities and defects; drug addiction; continued excessive or compulsive use of alcohol drinks; declared or undeclared war or civil strife; routine physical check-up and rest cures, or |
| 2. Cosmetic surgery for beautification purposes, or plastic surgery for any condition existing on the effective date of the insurance, except for the repair or alleviation of damage caused solely by accidental bodily injuries, or |
| 3. Treatment of Acquired Immune Deficiency Syndrome (AIDS) nor changes for the examination, immunization and detection of human immune deficiency virus and other related viruses, or |
| 4. Hospital confinement and charges caused by riot, civil commotion, war, invasion, act of foreign enemy, Hostilities (whether war be declared or not), civil war, rebellion, revolution, insurrection or military usurped power. Military or police operations against domestic rebellious groups, kidnapping or ransom groups. Military personnel activities are covered provided it is in line with duty; or |
| 5. Hospital confinement and charges caused ionizing radiations or contamination by radioactivity from nuclear waste from process of nuclear fission, or from any nuclear weapons material which is due to the profession or line of work of the insured, or |
| 6. The use or acquisition of special braces or prosthetic appliances such as artificial limbs, hearing aids and others but payable under Major Medical Benefits, or |
| 7. Any dental treatment or surgery, except dental operation to repair injury sustained in accident, or |
| 8. Treatments of any mental and nervous disorder such as psychosis, schizophrenia and others, any treatment arising from alcohol or drug addiction, or |
| 9. Any confinement for physical check-up or diagnostic purposes; treatment or surgical operations for congenital deformities such as harelip, clubfoot, cerebral palsy and others, for physical therapy; or for recuperative purposes such as confinement in a sanitarium or convalescent home, or |
| 10.Non-surgical care of tuberculosis and venereal diseases; or for treatment of communicable diseases such as small pox, cholera, bubonic plague, etc., Acquired Immune Deficiency Syndrome (AIDS) and other forms of complications attributed thereto, or |
| 11. Hospital services not in accordance with the diagnosis and treatment of the conditions for which hospital confinement is required, or |
| 12.Hospital confinement occasioned by or happening through pregnancy or childbirth with respect to women, or |
| 13.In the case of misstatement of age of which is not insurable at the time of enrollment, the benefit is not compensable, or |
| NOT COVERED ITEMS: | COVERAGE | GENERAL EXCLUSIONS | ||
| ALCOHOL | NOT COVERED | Unless exceptions to the following exclusions are made under the Benefits Provisions, this Memorandum Of Agreement shall not cover the following: | ||
| ARM BAND/ ID BAND/NAME TAG/WRIST BAND | NOT COVERED | A. | EXCLUSIONS SECONDARY TO SELF-CULPABILITY | |
| BEDPAN | NOT COVERED | 1 | Injury and its complications resulting from self-inflicted injuries including: | |
| CALIBRATED GLASS | NOT COVERED | · attempted suicide or self-destruction, whether sane or insane | ||
| COLD/ HOT WATER BAG | NOT COVERED | · infections as a result of tattoos, piercing on any body part aside from the ears, whether self- inflicted or done by a third party | ||
| DIAPER | NOT COVERED | 2 | Disabilities, injuries, or illnesses resulting from domestic violence; Healthcare Provider may rely on the Police or Doctor’s report to evaluate such claim. | |
| DIET PLAN/DIETARY/NUTRITION ASSESSMENT PLAN | NOT COVERED | 3 | Injuries or illnesses attributable to the individual’s own misconduct , gross negligence, vicious or immoral habit, including: | |
| DISTILLED WATER/ DRINKING WATER / MINERAL WATER | NOT COVERED | · unauthorized use of prohibited and regulated drugs | ||
| DRY SHEET / CURITY PAD | NOT COVERED | · alcoholic liquor intake | ||
| ELECTRICITY USED | NOT COVERED | · direct or indirect participation in the commission of a crime | ||
| ENVIRONMENTAL LEVY/WASTE DISPOSAL FEE | NOT COVERED | · violation of a law or ordinance | ||
| EXTRA BED / LINEN | NOT COVERED | · unnecessary exposure to imminent danger | ||
| EXTRA MEALS/FOODS | NOT COVERED | Healthcare Provider may rely on the Police or Doctor’s report to evaluate such claim. | ||
| EXTRA PILLOWS | NOT COVERED | 4 | Injuries or illnesses caused directly or indirectly by engaging in any risky sport or hazardous activity such as but not limited to handling firecrackers and explosives, scuba diving, boxing, mountain climbing, surfing, water-skiing, yachting, parachuting, drag racing, target shooting, motor sports, winter sports, skydiving, use of wood-working machinery | |
| FACE TOWEL / TOWEL | NOT COVERED | 5 | Illnesses resulting from exposure to ionizing radiation of any source | |
| FAMILY PLANNING | NOT COVERED | 6 | Injuries resulting from direct participation in any act of war and in state of civil, military, or political unrest (i.e. riots, strikes) | |
| FAX | NOT COVERED | 7 | Injuries or illnesses resulting from any combat-related activity or from participation in any political, police, investigative, firefighting activities while in military service | |
| FORMS/PHIC | NOT COVERED | 8 | Injuries resulting from conducting murder, assault, homicide or any attempt thereof, including injuries occasioned by provocation of the member | |
| HOSPITAL SERVICE FEE / MISCELLANEOUS CHARGES (UNSPECIFIED/NOT ITEMIZED) | NOT COVERED | B. | DIAGNOSTIC/THERAPEUTIC PROCEDURES AND MEDICATIONS NOT COVERED | |
| RISK ASSESSMENT / MEDICATION MANAGEMENT FEE | NOT COVERED | 1 | Routine physical examinations required for obtaining or continuing insurance, schooling, government licensing, health permit, travel documents, and other similar purposes, including routine PE for | |
| IV TRAY | NOT COVERED | employment (i.e. pre-employment PE, Annual PE) unless otherwise specified in the Schedule of Benefits | ||
| KIDNEY BASIN | NOT COVERED | 2 | All screening tests, including tests for Hepatitis screening | |
| MEASURING CUP | NOT COVERED | |||
| MEDICAL CERTIFICATE | NOT COVERED | |||
| MEDICAL RECORDS | NOT COVERED | 3 | Aesthetic, cosmetic, and reconstructive surgery or any consultation and treatment for beautification purposes, including varicose vein treatment (i.e. sclerotherapy, Endovenous Laser Therapy (ELT)), | |
| OFFICE FORMS | NOT COVERED | except if necessary to treat a functional defect due to accidental injury within the initial confinement | ||
| PHOTOCOPY | NOT COVERED | 4 | Treatment involving new diagnostic and therapeutic modalities such as but not limited to LASIK, | |
| PILLOWS | NOT COVERED | PET scan, physical therapy modalities (i.e. shockwave therapy, cold laser therapy, targeted radiofrequency, etc.) | ||
| PRIVATE NURSE | NOT COVERED | 5 | Experimental and/or investigational medical procedures and its complications | |
| RAZOR | NOT COVERED | 6 | Cost of intravenous immunoglobulin (IVIG), hyperalimentation, multivitamins and nutritional/food/herbal supplements, and vaccines for immunization, unless otherwise specified in | |
| RENT OF APPLIANCES (TV/REMOTE CONTROL/ELECTRIC FAN, ETC) | NOT COVERED | the Schedule of Benefits | ||
| SANITARY NAPKINS | NOT COVERED | 7 | Outpatient medicine and take-home medicine except chemotherapy medicine and medicine administered during an emergency treatment | |
| SLIPPERS | NOT COVERED | 8 | Cost of blood donor screening | |
| SPECIMEN CUP | NOT COVERED | 9 | Circumcision (except for treatment of phimosis), sex transformation, artificial insemination, | |
| SPOON & FORK | NOT COVERED | sterilization of either sex or reversal of such, and diagnosis, treatment and procedures related to fertility or infertility | ||
| TAKE HOME MEDICINES | NOT COVERED | 10 | Procedures for desensitization for hypersensitivity, including allergy testing, unless otherwise specified in the Schedule of Benefits | |
| TELEPHONE BILLS/CALLS | NOT COVERED | 11 | Hormone replacement therapy (HRT) for pre-menopausal or menopausal men/women or any other treatment for menstrual syndrome or menopausal syndrome | |
| THERMOMETER | NOT COVERED | 12 | Acupuncture, chirotherapy, and other forms of alternative medicine and their complications | |
| TISSUE / PAPER TOWEL | NOT COVERED | 13 | Cost incurred in the process of organ donation and transplantation, and its complications, if the member is the donor in such procedure/s | |
| TONGUE DEPRESSOR | NOT COVERED | C. | DISEASES/ILLNESSES NOT COVERED | |
| TRANSFER FEE | NOT COVERED | 1 | Psychiatric and/or psychological illnesses and conditions including but not limited to anxiety | |
| TUMBLERS | NOT COVERED | disorders (i.e. stress-related anxiety or anxiety attacks), psychotic disorders, bipolar disorders, depressive disorders, and personality disorders | ||
| UNDERPADS | NOT COVERED | 2 | Neurodevelopmental disorders including but not limited to: | |
| URINAL BAG/ WEE BAG | NOT COVERED | · Intellectual Disability (previously called mental retardation) | ||
| VITAMINS/ FOOD SUPPLEMENT | NOT COVERED | · Communication disorders (i.e. speech sound disorder) | ||
| CLAIMS PROCESSING / PROCESSING FEE | NOT COVERED | · Autism Spectrum disorder (i.e. Asperger’s disorder) | ||
| SCREENING | NOT COVERED | · Attention-Deficit/Hyperactivity Disorder (ADHD) | ||
| SHOE COVER | NOT COVERED | · Specific learning disorders | ||
| PPE | NOT COVERED | · Motor disorders (i.e. tic disorders, Tourette’s disorder) | ||
| ISOLATION GOWN/BLUE GOWN | NOT COVERED | · Cerebral Palsy, Epilepsy, Down syndrome, etc. | ||
| HEAD CAP | NOT COVERED | 3 | Congenital, genetic, hereditary diseases, and their complications, except if congenital benefits are covered as indicated in the Schedule of Benefits | |
| KN95 | NOT COVERED | 4 | Neonatal illnesses resulting from complications of pregnancy and delivery of the newborn infant | |
| JANITORIAL SERVICE | NOT COVERED | |||
| BEDDINGS | NOT COVERED | 5 | Maternity care and all other conditions related to and/or resulting from pregnancy and delivery including its complications, except if maternity benefits are covered as indicated in the Schedule of Benefits | |
| CLINICAL SERVICES (NURSING, MEDICAL TECHNOLOGIST, RADIOLOGY TECHNOLOGIST, ORDERLIE) | NOT COVERED | 6 | Obesity and its treatment including but not limited to bariatric surgery, liposuction, weight reduction programs, etc. | |
| DIETARY SERVICES | NOT COVERED | 7 | Sleep Disorders and Eating Disorders | |
| SECURITY SERVICES | NOT COVERED | 8 | Error of refraction, including diagnostic procedures and treatment, except consultation | |
| MAINTENANCE FEE (ELECTRICAL/MECHANICAL) | NOT COVERED | 9 | Chronic Dermatoses such as: | |
| HOUSEKEEPING | NOT COVERED | · Chronic Idiopathic and/or Psychogenic Dermatoses (i.e. acne, alopecia areata, psychogenic purpura, rosacea, chronic urticaria) | ||
| COMMUNICATION FEE | NOT COVERED | · Primary Psychiatric Dermatologic disorders (i.e. bromosiderophobia, delusion of parasitosis, dysmorphophobia, factitial dermatitis, trichotillomania) | ||
| RT-PCR TEST (UPTO 1 ONLY TEST ONLY OF PATIENT) | NOT COVERED | · Autoimmune and Hormonal Dermatoses (i.e. ichthyosis, psoriasis, vitiligo, atopic dermatitis, seborrheic dermatitis | ||
| 10 | Demyelinating diseases of the nervous system (i.e. multiple sclerosis), Autoimmune neurologic disorders (i.e. myasthenia gravis, Guillain Barre syndrome), and Neurodegenerative diseases (i.e. Alzheimer’s disease, Parkinson’s disease) | |||
| 11 | Sexually transmitted infections (STIs) including but not limited to condyloma acuminata, genital warts, gonorrhea, chlamydia, molluscum contagiosum, syphilis, trichomoniasis, etc. | |||
| 12 | HIV infection, AIDS, and their complications; Suspected HIV infection (subject to medical evaluation by the Healthcare Provider or unless proven otherwise by member through submission of a valid negative HIV test result) | |||
| 13 | Dental-related condition or illnesses, including its complications (i.e. maxillary sinusitis of odontogenic origin), except if dental benefits are covered as indicated in the Schedule of Benefits | |||
| 14 | Injuries or illnesses attributable to third party liabilities, if Member refuses to execute a Deed of Subrogation and Reimbursement | |||
| Diseases that are declared epidemic or pandemic by the Department of Health, World Health Organization, or any recognized health authority (i.e. Avian flu, Meningococcemia, etc.) | ||||
| 15 | ||||
| 16 | Pre-existing medical conditions or illnesses unless otherwise specified in the Schedule of Benefits | |||
| D. | MISCELLANEOUS EXCLUSIONS | |||
| 1 | Custodial, domiciliary, convalescent and intermediate care | |||
| 2 | Professional fees for medico-legal cases; Professional fees of assistant surgeons except when the | |||
| service of an assistant surgeon is medically necessary, subject to the approval of the Healthcare Provider | ||||
| 3 | Benefits covered by PhilHealth and all other government funded healthcare entitlements as provided | |||
| for by law | ||||
| 4 | Charges for non-medical services such as those of private duty nurses or physicians; charges for non-medical amenities such as telephone, radio, television, refrigerator, extra bed/ beddings, | |||
| toiletries and the like unless these are included in the Member’s room and board accommodation | ||||
| 5 | Purchase or use of durable medical equipment such as but not limited to oxygen dispensing unit, except if rented while confined at the hospital | |||
| 6 | Cost of corrective/prosthetic appliances, artificial aids, surgically implanted external devices, orthopedic hardware, and hearing aids and its fitting | |||
| 7 | Cost of hospital confinement wherein the Member went home against medical advise (HAMA), or was discharged against medical advise (DAMA), or has absconded, including succeeding availments for the same illness, subject to the approval of the Healthcare Provider |
| PRE-EXISTING MEDICAL CONDITIONS |
| An illness is considered to be pre-existing if any of the following conditions are present: |
| 1. Such illness or condition was, in any way, evident to the Individual before the effective date of the Memorandum of Agreement. |
| 2. Any professional advice or treatment for such illness or condition was obtained prior to the effective date of the Memorandum of Agreement. |
| 3. The pathogenesis of such illness or condition has started prior to the effective date of the Memorandum of Agreement, whether or not the Individual is aware of such illness. |
| 4. Illnesses or conditions disclosed in the application form. |
| The following, among others, when occurring within the first 12 months of coverage, are considered as Pre-existing Conditions: |
| PRE-EXISTING NON-DREADED CONDITIONS |
| 1. Anal Fistulae |
| 2. Benign Prostatic Hypertrophy |
| 3. Calculi of the urinary tract, kidney, and gallbladder (except choledocholithiasis and other stones in the biliary tract) |
| 4. Endometriosis, simple ovarian cyst (10 cm (excluding ruptured ovarian cyst), Polycystic |
| Ovarian Syndrome (PCOS) |
| 5. Uncomplicated hypertension (essential/primary hypertension alone) |
| 6. Gastritis, duodenitis, uncomplicated gastric/duodenal ulcer (non-bleeding ulcers) |
| 7. Hemorrhoids |
| 8. Hernia (unless congenital) |
| 9. Non-toxic goiter |
| 10. Migraine headache |
| DREADED CONDITIONS are defined as “generally chronic and irreversible” diseases that require frequent and/or prolonged hospitalization. |
| PRE-EXISTING DREADED CONDITIONS |
| 1. Arthritis (such as rheumatoid arthritis, osteoarthritis, chronic gouty arthritis) |
| 2. Benign or malignant new growth |
| 3. Blood dyscrasias (such as leukemia, idiopathic thrombocytopenic purpura) |
| 4. Cataract and glaucoma |
| 5. Cerebrovascular diseases (such as stroke, aneurysm, etc.) |
| 6. Choledocholithiasis and other stones in the biliary tract (except in the gallbladder) |
| 7. Chronic cardiovascular diseases (such as aortic dissection, abdominal aortic aneurysm, myocardial infarction, congestive heart failure, coronary artery disease, cardiomyopathies, valvular heart disease, cardiac arrhythmias, and peripheral vascular disease) |
| 8. Chronic EENT diseases (such as chronic otitis media, primary acquired cholesteatoma) |
| 9. Chronic endocrine disorders (such as diabetes, dyslipidemia, hormonal dysfunctions, thyroid dysfunctions except non-toxic goiter) |
| 10. Chronic gastrointestinal diseases (such as irritable bowel syndrome, Crohn’s diease) |
| 11. Chronic genito-urinary disorders |
| 12. Chronic kidney diseases |
| 13. Chronic liver parenchymal diseases (such as liver cirrhosis, chronic hepatitis, non-alcoholic fatty liver disease/steatohepatitis) |
| 14. Chronic pulmonary diseases (bronchial asthma, chronic obstructive pulmonary diseases such as emphysema, chronic bronchitis) |
| 15. Collagen, connective tissue, immunologic disorders |
| 16. Muscular dystrophy (such as Duchenne, Becker, limb-girdle dystrophy) |
| 17. Secondary hypertension (such as hypertension sec. to chronic kidney disease) and hypertension with complications (such as HCVD, HASCAD, hypertension and CVD or stroke, hypertension with co-existing diabetes) |
| 18. Tuberculosis, pulmonary and extrapulmonary |
| 19. All complications resulting from above list of conditions |
| 20. Any pre-existing illness other than above which would require prolonged hospitalization and/or critical care or confinement to intensive care unit |
| CATHASTROPIC ILLNESSES are defined as any illness, other than pre-existing dreaded illnesses, requiring prolonged hospitalization or recovery, usually life-threatening, and may leave residual disability. |
| PRE-EXISTING CATHASTROPIC ILLNESSES |
| Injuries or illnesses due to or caused by accident requiring major surgery and prolonged hospitalization |
| for more than 14 days. (Occupational, Vehicular Accident, Fall, Accidents cause by Natural calamities, and Accidents with Third-Party involvement) |
| Burns requiring Intensive care, Isolation, skin grafting and hospitalization for more than 14 days. |
| *Conditions considering the contestability period for new members (3 months, 6 months, 12 months) |